

What you should know about hip labral tears in young athletes
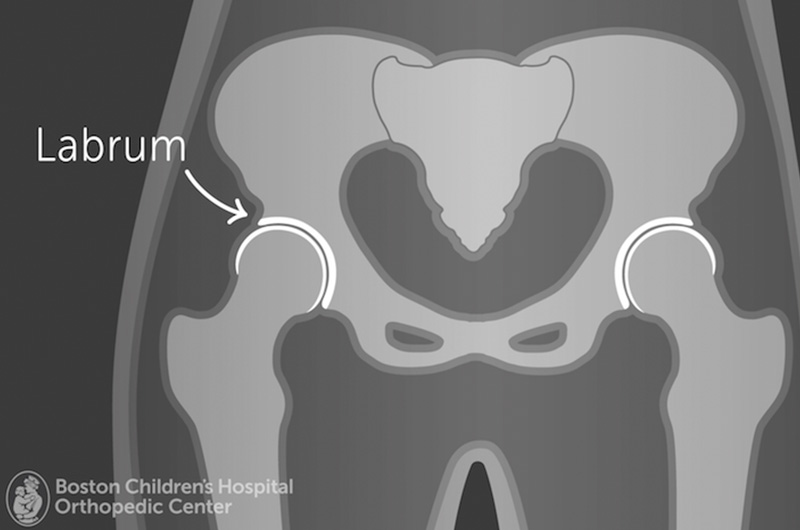
Labral tears are a common injury of the hip, particularly with young athletes who may have underlying hip anatomy issues, such as hip dysplasia or impingement. Treatments for labral tears range from rest and physical therapy to open surgery. Recovery (and time away from sports) can take days, weeks, or even months.
It’s important that anyone with hip pain see a physician as soon as possible in order to limit pain and damage to the hip. Dr. Young-Jo Kim, a pediatric and young adult orthopedic hip specialist and director of the Child and Young Adult Hip Preservation Program at Boston Children’s Hospital, discusses the causes of labral tears and his treatment philosophy.
When you see a patient who has labral tear, how does that appointment usually go?
If I see a new patient, I usually start out with their history and a physical. I’ll ask them, “How did this injury happen? Where is the pain located? What makes it hurt more?” If it’s an athletic injury, the pain could have started pretty suddenly, but more often, the onset of pain is gradual.
Hip impingement is friction in the hip joint caused by abnormal contact between the femur and acetabulum.
Certain sports and activities may predispose people to labral tears. It’s more common among athletes who do a lot of rotating and twisting leg motions, such as golf, soccer, ice hockey, ballet, and football.
What kinds of athletes do you see most often for this injury?
I see labral tears most often in hockey players — particularly goalies — and dancers. These athletes seem to put unique stress on their hips, and labral tears are quite common, unfortunately.
What is the difference between a labral tear in a younger person versus an adult?
When people are older, they can get labral tears just from the wear and tear of aging. But if you are talking about someone in their teens or early 20s, the injury is often the result of activity. In many cases, it’s also due to certain issues of anatomy, such as hip dysplasia or impingement. The majority of the patients I see have some sort of underlying issue with the shape of their hip joints.
Would you say that’s the main driver behind labral tears or hip pain?
That’s the current thinking — that there’s some susceptibility to labral tears from problems in the underlying hip anatomy. Combined with the demands an athlete may put on their hip, this can damage the labrum.
When you see patients who have hip anatomy issues along with a labral tear, do you usually suggest surgery?
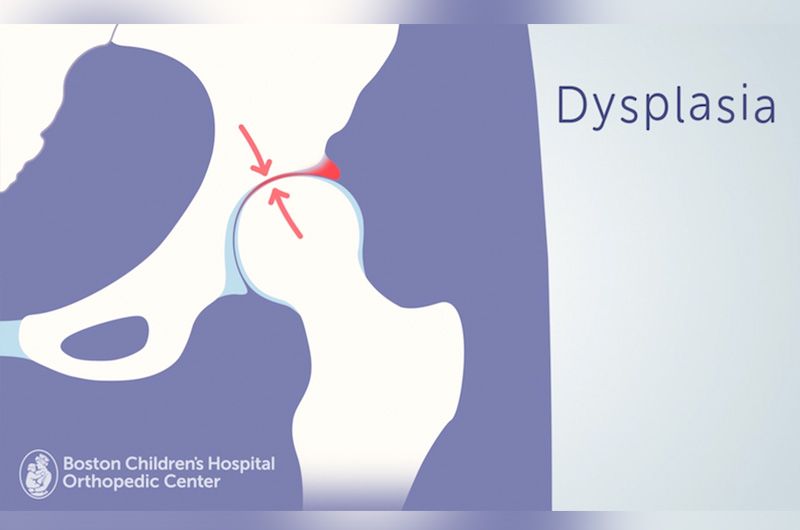
If they have hip dysplasia and a labral tear, which is a common combination, we talk about most likely needing to fix the dysplasia surgically. For a person with hip dysplasia, their hip socket is too shallow and the labrum is not well supported. If you just fix the labral tear, it can often re-tear. If we were to do surgical treatment, we would try to fix the underlying cause as well as the labral tear.
We do a lot of nonsurgical management, however, especially with patients who have small labral tears and minimal or no hip anatomy issues. We work closely with the sports medicine primary care physicians here at Boston Children’s to help patients get the best access to therapy.
Some athletes not only have a labral tear as well as a lot of tendonitis around the hip. In that case, we would do therapy and injections to try to calm that down. What’s nice about our Sports Medicine Division is that Drs. Pierre d’Hemecourt, Andrea Stracciolini, and Sarah Jackson know a lot about therapeutic hip treatments. They’re also the ones who do ultrasound exams and injections. We have complementary skills.
If a patient has underlying anatomical hip problems, do you suggest surgery right away, or do you try nonsurgical options first?
There’s a spectrum. If an athlete comes in with a labral tear and has mild hip dysplasia, we will try treating them without surgery first. If their symptoms improve, I will let them return to sports, but advise them that the labrum can re-tear. If they have symptoms of another labrum tear, they should come back for further treatment, and it will likely be surgical.
If a patient has severe dysplasia or impingement, I’ll offer nonsurgical treatment, but it often does not work. That’s a discussion between me and the patient.
In general, I think of each patient’s condition and injury as unique. There isn’t going to be one best answer for every patient. Our shared decision-making is based on each patient’s situation and what’s best for that person.
Learn more about Boston Children’s Child & Young Adult Hip Preservation Program.
Related Posts :
-

A rare injury, a more determined player: Adrian’s knee dislocation
Adrian can barely remember a time when he didn’t play football. Now 16, he grew up watching games with his ...
-
How a meniscal transplant made me a Boston sports fan
I was in kindergarten when my knee started popping and cracking. My parents and I didn’t know it at ...
-
Hard and beautiful at the same time: Five lessons of raising a medically complex child
When they learned they were expecting a baby, Michelle and Stephen Strickland were delighted. The South Carolina couple looked forward ...
-
3D imaging could become standard practice in orthopedics. Here’s how.
It took a trained eye to see the abnormality on the patient’s X-ray. There, hidden behind the acetabulum was ...



