

Predicting brace adherence could change the game in scoliosis treatment

When it comes to preventing scoliosis progression, is it possible to make bracing more effective? For decades, spine specialists focused on improving the braces themselves, making them lighter, less obtrusive, and easier to put on and take off. (The Boston Brace, developed at Boston Children’s Hospital in the early 1970s, is one example.)
Key takeaways
- Patients who adhered to bracing protocol in the first month continued to adhere up to 24 months later.
- Progression from moderate to severe scoliosis was more common in the nonadherent group.
- Curve correction was more likely among patients in the adherent group.
With the addition of built-in sensors that indicate how many hours a brace was worn, two things became clear. One: Despite improvements in brace design, many patients wore their braces far less than they thought or said they did. Two: Patients who wore their braces more had better outcomes.
If a spine specialist could predict which patients were least likely to adhere to a bracing regimen, could they reduce the number who eventually need spinal fusion surgery? Would it be possible, in fact, to increase the rate of curve correction through bracing alone?
Timothy Hresko, MD, director of spine research and quality improvement in Boston Children’s Spine Division, believes the answer to both of these questions is yes.
Predicting who will and who won’t wear a brace
As he read reports linking hours in a brace to curve stabilization, Hresko started to rethink the field’s approach to moderate scoliosis. Rather than continually trying to improve brace designs, he thought, “maybe it’s time to shift our focus to helping kids accept the fact that they need to wear the brace.”
But first, spine specialists would need to know more about patterns of adherence. Do patients who initially resist wearing a brace eventually come around? Or does a patient’s early acceptance or nonacceptance of bracing indicate how they’re likely to behave in the future?
In a study published in Spine, Hresko and his colleagues analyzed brace adherence in 60 patients with adolescent idiopathic scoliosis over two years. Patients fell into one of two groups, adherent — defined as wearing the brace for at least 80 percent of the hours prescribed — and nonadherent.
At their one-month follow-up visit, 32 patients met the criteria of adherence. By the time of their six-month visit, these patients had worn their braces an average of five hours more per day than those in the nonadherent group. This pattern continued throughout the 24 months studied. Those who started out wearing their braces the most continued to do so while those who resisted wearing a brace early on did not adapt to the treatment regimen over time.
From scoliosis stabilization to correction
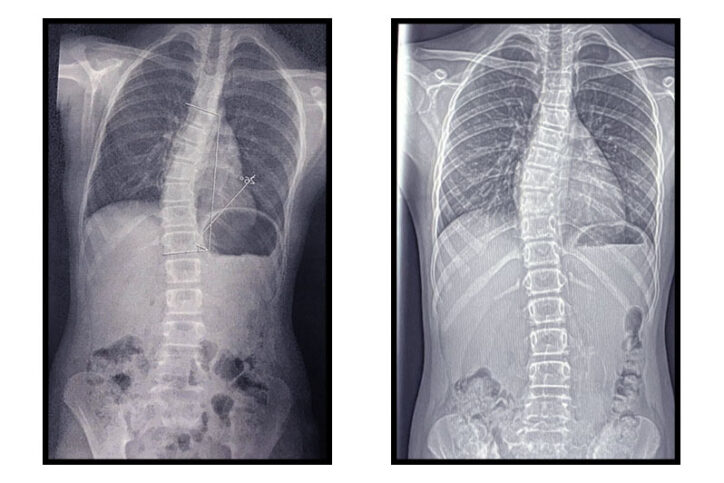
In keeping with previous studies, bracing was far more successful among patients in the adherent group, with only one progressing to severe scoliosis (a Cobb angle greater than 40 degrees). By contrast, seven patients in the nonadherent group progressed from moderate to severe scoliosis. Further, patients in the adherent group showed significant curve reduction.
These results, says Hresko, are reason to change the way spine specialists talk about scoliosis and bracing with patients.
Up until now, patients with moderate scoliosis have typically been told that wearing a brace may prevent their curve from progressing but they shouldn’t expect it to cure their scoliosis. By contrast, Hresko presents bracing as an opportunity for patients to take charge of their lives. “It’s crucial that patients are actively involved in their own care,” he explains. “If they’re passive, if someone else is making them wear the brace, it’s a lot less likely they’ll be adherent.”
The future of bracing adherence
Hresko considers adherence a game changer in scoliosis treatment. “There’s a large group of adolescents with scoliosis who can reduce the chance they’ll need surgery by spending more hours in their brace,” he says.
To understand how to best reach them, Hresko and his team are planning a prospective study that will analyze factors — familial, social, personal — driving adherence or nonadherence. Ultimately, they plan to use the results to help more patients with scoliosis reach a place at which wearing a brace is a choice they make for their own well-being.
Learn more about the Spine Division or make a referral.
Related Posts :
-

How Josie’s bad day turned into a campaign to help kids with scoliosis
Josephine DeFilippi (Josie) describes the day of her scoliosis diagnosis as the hardest day of her life. Right when she ...
-
Scoliosis bracing: How to support your child
Q&A with M. Timothy Hresko, MD and Deborah Cranford, RN Most patients with idiopathic scoliosis will never need ...
-
A modified brace and a new treatment option for infantile scoliosis
While bracing is a common treatment for adolescents with moderate idiopathic scoliosis, infantile scoliosis is typically treated with casting. But ...
-
A new treatment option for Jeanne’s infantile scoliosis
If it hadn’t been for the pandemic, Jeanne McDaniel’s treatment for infantile scoliosis would have started when she ...



